Lessons of Space Catastrophes
An in-depth analysis of five fatal space disasters — Apollo 1, Soyuz 1, Soyuz 11, Challenger, and Columbia — that killed 21 people, examining the systemic failures behind each and the bitter lessons learned.
In total, five space catastrophes have occurred — incidents resulting in the death of cosmonauts or astronauts during spacecraft operation in space or during preparation for flight. In these five incidents, twenty-one people died. Today we'll examine what happened and what lessons were learned.
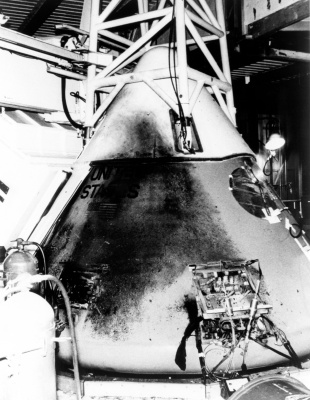
Apollo 1

Crew: Gus Grissom, Ed White, Roger Chaffee
The lunar race between the USSR and USA drove rapid Apollo spacecraft development. The Command Module existed in two versions — Block I for unmanned testing and Earth orbit flights, and Block II for lunar missions. Two successful unmanned flights (AS-201 and AS-202) occurred in 1966, with the first crewed mission planned for late February 1967.
On January 27, 1967, the crew was undergoing a plugs-out integrated test — a simulation of command module operation on internal power. The test was considered safe: fuel tanks were empty, pyrotechnic devices were disabled. However, the test encountered numerous communications problems and progressed slowly.
At 18:30:54, voltage fluctuations were detected in telemetry. At 18:31:04, Chaffee exclaimed "Hey!" and scraping sounds were audible. At 18:31:06, White reported: "Fire in the cabin!" Flames were visible moving left to right; smoke obscured television screens. At 18:31:12, "We've got a bad fire!" was heard, followed by module rupture sounds and cries. At 18:31:21, audio transmission ceased. Around 18:36, ground personnel reached the module and opened the hatches; smoke filled the interior.

An electrical spark or short circuit initiated the fire, likely from worn insulation or static electricity. However, multiple contributing factors were identified.
The crew could not rapidly exit due to the hatch design — it consisted of two parts (the upper one opened outward, the lower one inward). Pressure from heating made the inner hatch impossible to open. The absence of an emergency hatch release system stemmed from concerns about unauthorized activation, referencing Grissom's near-fatal experience in 1961 when his capsule's hatch spontaneously ejected post-splashdown.
The pure oxygen atmosphere at above-atmospheric pressure (16 psi or 1.1 atm) intensified combustion. Materials normally non-flammable burned readily — including aluminum. NASA had successfully employed this atmosphere on Mercury and Gemini spacecraft, allowing weight savings and simplified life support, creating complacency about fire risks.
Corrective actions:
- Launch atmosphere modified to 60% oxygen, 40% nitrogen
- Hatch redesigned to open outward
- Combustible materials replaced with non-flammable alternatives (nylon replaced with fiberglass "Beta-cloth")
- Wiring insulated with non-flammable material (Teflon)
- 1,407 wiring problems corrected
The Apollo program experienced a 20-month delay. Subsequent vehicles demonstrated excellent reliability; the serious Apollo 13 incident caused no fatalities.
Soyuz 1
Crew: Vladimir Komarov
This ambitious mission planned simultaneous launches of Soyuz 1 (Komarov) and Soyuz 2 (Belyayev, Yeliseyev, Khrunov). The vehicles were to dock, with two cosmonauts transferring via EVA to Soyuz 1. Multiple systems failed immediately after launch: one solar panel failed to fully deploy, the ion orientation system operated erratically, and the sun-star orientation sensor malfunctioned.
Asymmetrical panel deployment shifted the center of mass, preventing adequate sun-oriented spin for battery charging and causing orientation system problems. Mission termination became necessary. Return operations encountered additional difficulties — system failures and asymmetrical mass distribution prevented proper retrofire orientation. Mission Control developed emergency orientation procedures; Komarov manually oriented the vehicle correctly, executed proper braking impulse, separated the modules, and descended through the dense atmosphere.

At 9.5 km altitude, the main parachute compartment hatch ejected and the drogue chute deployed to extract the main parachute. But the main parachute failed to deploy — it remained stuck in the container. At 5.5 km altitude, the reserve parachute automation detected unacceptable descent rate and activated the reserve chute. But the reserve parachute remained shadowed by the drogue and failed to inflate. Impact occurred at approximately 140 km/h. Concentrated hydrogen peroxide remaining in the tanks (used for descent control) ignited intensely, further complicating the investigation.
The main parachute failure resulted from insufficient drogue parachute force. Two possible causes emerged:
Manufacturing process violation: The descent apparatus was placed in an autoclave for thermal resin polymerization. However, parachute container covers arrived late and were autoclaved separately. Inadequate covering allowed volatile coating compounds to contact the container walls, creating rough, bumpy, adhesive surfaces. Increased friction made the drogue parachute force insufficient to pull out the main chute.
Design error: Due to schedule pressure, Soyuz never completed a normal landing before Komarov's flight. The unmanned Cosmos-133 was destroyed during descent to prevent a potential non-Soviet territory landing. Vehicle 7K-OK No. 1 landed on its reserve parachute due to incorrect emergency system activation. Cosmos-140 descended depressurized due to heat shield perforation. A normal landing would have pressurized the descent apparatus, compressing the container and reducing drogue parachute effectiveness — a problem that was never observed because a normal landing never occurred.
The reserve parachute failure resulted from aerodynamic shadowing by the drogue parachute. Investigation revealed this failure scenario was never tested.
Ironically, the solar panel deployment failure (which snagged on insulation), derailing the mission, saved the lives of Belyayev, Yeliseyev, and Khrunov — who were scheduled to fly on the identical, fatally-flawed vehicle.
Corrective actions:
- Main parachute container redesigned: increased rigidity, expanded volume, modified shape, and internal polishing
- Each parachute system assembly operation photographed for quality control
The Soyuz program experienced an 18-month delay. Six developmental unmanned flights preceded the next crewed mission. No subsequent parachute system problems occurred.
Soyuz 11

Crew: Georgy Dobrovolsky, Vladislav Volkov, Viktor Patsayev
By 1971, the Soviet Union had lost the lunar race but responded asymmetrically by developing orbital stations for extended research. The first expedition to the world's first orbital station was nearing completion after 23 days of successful operations.
The crew transferred to Soyuz 11 and undocked from the station. Retrofire and descent proceeded nominally, but after module separation, communication was lost. The descent capsule landed successfully, but the crew was found unresponsive. Resuscitation efforts failed.
Here's what happened: at 01:47:28 Moscow time, at 150 km altitude, module separation occurred via pyrobolt detonation. Simultaneously, a ventilation valve — designed to open only at 2-3 km altitude — spontaneously opened. The cabin fogged as water vapor condensed from the pressure loss. The hissing of escaping air was audible. The cosmonauts disabled the radio to locate the leak by ear. Dobrovolsky (some sources cite Patsayev) unstrapped from his seat and attempted to close the valve, but selected the wrong one — two separate valves existed, each with individual manual controls. Approximately 20 seconds later, the cosmonauts lost consciousness. Within 115 seconds total, cabin pressure dropped to 50 mmHg. Death resulted from asphyxiation.

Spontaneous ventilation valve opening during module separation was not definitively established as a cause. Proposed theories included:
Assembly process violation: Internet accounts (without authoritative sources) describe inadequately tightened fasteners or completely loose hardware. While unconfirmed, this represents the most likely scenario within technologically complex manufacturing industries.
Shock wave from pyrobolt detonation: The investigation commission proposed this theory, but extensive barometric chamber experiments failed to reliably reproduce the effect.
Systemic design errors compounded the catastrophe. The Soyuz design principle stated: "Any single system failure must not compromise mission success; any second failure must not endanger crew life." This principle was violated with the ventilation valve — without spacesuits, a single valve failure became fatal.
For seven years, cosmonauts and military air force representatives had requested spacesuits; engineers dismissed these requests. The absence of depressurization incidents was used as evidence of system reliability. The forced exclusion of spacesuits on Voskhod 1 (three cosmonauts couldn't fit otherwise) became normalized, and Soyuz spacecraft were designed without them from inception.
The necessity and operational logic of the ventilation valve were questionable. These valves addressed the scenario of capsule inversion during landing, when the hatch couldn't open. They activate automatically at 2 km, with manual override for water landings. Nobody considered designing manually-operated valves without automation.
Control interface ergonomics were poor. Accessing the valve control levers required unstrapping from the seat — demanding time and making emergency access impossible under acceleration.
Accusations that "the hole could have been plugged with a finger" were baseless; the valve was panel-mounted with no direct access.
Corrective actions:
- Spacesuits and oxygen systems reinstalled on all subsequent flights
- Control interfaces redesigned for improved ergonomics
- This required reducing the crew to two temporarily, though rocket improvements eventually permitted three-person crews again
The program halted for 27 months. Subsequently, Soyuz has operated successfully for over 40 years, justly earning a reputation for exceptional reliability.
Challenger STS-51-L

Crew: Richard Scobee (Commander), Michael Smith (Pilot), Judith Resnik, Ellison Onizuka, Ronald McNair, Gregory Jarvis, Christa McAuliffe (Payload Specialist)
The years 1984-1986 represented the Space Shuttle program's "golden age" — first reusable rocket pack flights, initial orbital satellite repair, first damaged satellite recovery in the cargo bay, 23 satellites and 142 tons of payload deployed in two years. Rapid launch schedules (April 1985: launches separated by only 17 days) set records. Challenger's STS-51-L mission was planned just 16 days after STS-61-C. Simultaneous launch complex preparations made Kennedy Space Center resemble imagery from science fiction. The mission featured a schoolteacher conducting orbital lessons — intended to revive public interest in NASA amid its diminished profile. Media showed only the initial launch seconds before reverting to standard programming. Within minutes, emergency broadcasts reported the shuttle's destruction along with the crew.
Sequence of events:
- T+0.678s: Black smoke clouds observed from right solid rocket booster near the lower attachment node; booster sections joined with smoke emanating from the joint
- T+3.375s: Smoke ceased
- T+58.788s: A flame torch became visible from the lower right booster
- T+64.660s: The flame penetrated the external tank wall; liquid hydrogen leaked, intensifying the torch via burning hydrogen
- T+72.284s: The right booster's lower attachment point failed
- T+73.124s: The lower (hydrogen) tank bottom ruptured; sudden acceleration forced the lower tank upward, striking the upper (oxygen) tank, while the pivoting right booster struck the external tank. External tank destruction accelerated through component combustion
- T+73.162s: Orbiter destruction commenced
- T+75.237s: The orbiter cabin separated from the debris clouds; the astronauts remained alive and conscious. Three of four personal air supply units were activated. Cockpit switches were manually manipulated, indicating attempts to restore electrical power and control
- T+240s: The cabin struck the ocean at 330 km/h; the astronauts perished
Gas leakage through solid rocket booster segment connections caused the immediate failure. Seal degradation had been documented since STS-2 (Challenger was the 25th flight). Initial testing following the STS-2 incident involved intentional seal damage exceeding STS-2 failure severity, subjected to three times normal operating chamber pressure. The seal held. However, this test proved inadequate. From 1984 to 1988, 18 missions revealed seal problems in only three cases. More critically, 9 of 15 affected missions experienced gas breakthrough.
Engineers understood the problem's severity but lacked resources for thorough investigation and remediation. The brilliant visible success of NASA masked catastrophic personnel overload. Astronaut Mike Mullane's memoir describes teams working months without rest days, workers summoned evenings from home, some performing duties intoxicated. NASA procurement documents overflowed with unfulfilled requests for personnel, parts, and equipment — budget insufficiency prevented acquisition. The Space Shuttle program's economic projections proved dangerously flawed; self-funding never materialized while appropriations proved inadequate.
Information distortion within organizational hierarchies worsened the situation. Managers unjustifiably minimized accident probability based on crewed vehicle status, ignoring escalating warnings. The evening before Challenger's launch, Thiokol and NASA representatives held a conference. Engineers, sensing that low temperatures might further compromise seal integrity, advocated launch postponement for warmer conditions. NASA management responded: "My God, Thiokol, where do you want to launch this, in April?"
The astronauts' deaths resulted from water impact. Although the cabin survived orbiter destruction and fell intact with living astronauts aboard, no emergency escape system existed for first-stage failures (before solid rocket booster separation). Early missions with two-person crews featured ejection seats; after operational-status declarations expanded crews to seven, the seats were removed. The Space Shuttle program generally displayed engineering overconfidence — notably exemplified by the very first crewed mission.
Corrective actions:
- Solid rocket booster connections redesigned with an additional sealing ring and reinforced coupling elements
- A primitive escape system installed, operational only for intact, controlled shuttles with nowhere to land — reminiscent of WWII-era technology (conventional parachute and guide rod preventing contact with the orbiter's wings)
Space Shuttle flights halted for 32 months. A fifth orbiter, Endeavour, was constructed to replace Challenger. Concurrent unmanned launch failures and the Hubble Space Telescope optical defect created a cascading NASA crisis. Some proposals advocated the agency's dissolution.
Columbia STS-107

Crew: Rick Husband (Commander), William McCool (Pilot), Kalpana Chawla, David Brown, Michael Anderson, Ilan Ramon, Laurel Blair Salton Clark
By 2003, the late-1980s crisis appeared to have been overcome. Shuttles no longer represented the sole orbital cargo delivery system. Dangerous reusable rocket pack operations were cancelled. The Hubble underwent successful orbital repair. International Space Station construction proceeded actively. Columbia, the first-built orbiter and structurally too heavy for ISS assembly missions, conducted scientific missions via SpaceHab modules. The January 16 launch appeared superficially successful; thermal insulation foam again detached — a routine observation. Orbital operations concluded successfully. The loss of a left wing tire pressure sensor was treated as a typical mission anomaly. Communication loss provoked minimal concern. Houston Mission Control was still attempting signal recovery when a control room employee observed televised imagery showing atmospheric vehicle disintegration.
Sequence of events:
- January 16, 2003, 83 seconds post-launch: A foam insulation chunk the size of a briefcase struck the left wing
- February 1, 2003, 8:44:09 EST, Entry Interface (EI)+000: Atmospheric entry interface point at 120 km altitude
- EI+404: Peak heating period commences (10-minute duration). Velocity 24.1 Mach; altitude 74 km
- EI+597: First debris shedding observed. Velocity 22.8 Mach; altitude 70.2 km
- EI+613: Telemetry shows four left wing temperature sensors registering beyond minimum scale — actually burned through
- EI+906: Left landing gear pressure data lost
- EI+923: Communication and telemetry transmission ceased
- EI+969: Amateur video documented the shuttle's destruction
- EI+1710: Mission Control learned of the destruction via television broadcast
Left wing leading edge damage from the foam strike during ascent caused the failure. The precise damage dimensions remain unknown — engineers never seriously investigated, and despite available ground telescopes and reconnaissance satellites, no examination occurred. Foam strikes were considered routine and harmless. Experimental modeling later indicated substantial perforation ensuring orbiter destruction.
The astronauts' deaths resulted from high-velocity atmospheric disintegration. Mary Roach's "Packing for Mars" obliquely references unusual trauma from hypersonic shock effects. Current technology provides no rescue capability under such conditions.
Two potential rescue scenarios existed:
Coincidentally, Atlantis was launch-ready. Columbia could have remained in orbit until February 15 with sufficient resources; Atlantis could have launched February 10 without formal system testing — providing five days for rescue and possible orbiter recovery.
As an alternative, the crew could have conducted EVA for damage assessment and repair attempts. While Columbia lacked the Canadarm manipulator normally used for EVA support, spacesuits were aboard every shuttle flight precisely for emergency repairs. While successful orbiter repair remained uncertain, any attempt exceeded the alternative of accepting guaranteed destruction.
Essentially, the investigation commission's Challenger recommendations were ignored. Columbia demonstrated identical patterns: a potentially dangerous phenomenon emerges repeatedly without catastrophic results, habituation follows, insufficient countermeasures are activated, and eventual catastrophe occurs.
Corrective actions:
- Foam shedding problem resolution took three years post-Columbia. Multiple shuttle missions continued experiencing foam ejections. Only X-ray tank examination revealed stress cracks causing foam fragments. Even 2006's STS-121 mission shed foam
- ISS-bound shuttle missions implemented new procedures: orbital position near ISS with rotation for thermal tile documentation via ISS crew photography
Space Shuttle flights were suspended for 29 months. The Columbia disaster effectively terminated the Space Shuttle program. Post-catastrophe missions accomplished only mandatory ISS assembly and Hubble servicing before permanent retirement.
Bitter Lessons
All five catastrophes were entirely preventable — none resulted from unconquerable external forces, pure chance, or crew error. Seven critical lessons emerge:
- Familiar danger doesn't become safer. Well-known hazards demand vigilant attention equal to unfamiliar ones.
- When solving one problem, avoid creating its opposite. Corrective measures may introduce opposing risks.
- Demanding faster work shouldn't surprise you when people cut corners covertly. Schedule pressure severely compromises quality.
- Rushing toward completion may necessitate extensive disaster remediation. A motivation for deliberate, methodical progress.
- Negligent risk management or test case development may produce significant losses. Omitted risks or scenarios painfully emerge during operation.
- Thinking like "not a bug, it's a feature" killed fourteen people in space. Non-conforming behavior without catastrophic consequence provides no guarantee of future safety.
- Ignoring mistakes means repeating them perpetually.
These lessons are not confined to space. They extend naturally to information technology and project management, where bugs, failures, and deadlines prove universally applicable. As Boris Chertok wrote in his remarkable "Rockets and People" — a book that parallels Eliyahu Goldratt's "The Goal" — these patterns repeat across all complex engineering endeavors.